- Sexually-coercive behaviors, like when a person:
- pressures or forces a sexual partner to have sex when s/he doesn’t want to have sex;
- threatens to end a relationship if a person doesn’t have sex;
- forces a sexual partner to not use birth control, including a condom, contraceptive pills, or other available options;
- intentionally exposes a sexual partner to a sexually-transmitted infection (STI); or
- retaliates against a sexual partner when told about a positive (STI) result.
- Birth control sabotage, like when a person:
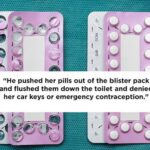
- hides, withholds, or destroys a sexual partner’s birth control pills;
- replaces or tampers with a sexual partner’s birth control pills without the partner’s knowledge or consent;
- breaks or pokes holes in a condom on purpose;
- removes a condom during sex without telling his/her sexual partner;
- refuses to withdraw during sex, even if s/he previous agreed to do so;
- pulls out a sexual partner’s vaginal contraceptive ring; or
- tears off a sexual partner’s contraceptive patch.
- Pregnancy pressure, which is when a person pressures a sexual partner to:
- get pregnant when s/he doesn’t want to be pregnant;
- continue a pregnancy when s/he wants an abortion; or
- end a pregnancy s/he wants to continue.
Even if your sexual partner has not done any of the specific things listed above but is controlling your reproductive choices in other ways, you may still be experiencing reproductive abuse or coercion. If you think your partner is trying to control your reproductive choices, you may want to contact a domestic violence advocate for
- buying birth control or condoms on your own, instead of allowing your partner to buy it;
- keeping birth control or condoms in a hidden or private location;
- inspecting birth control pills to make sure they are the correct pills;
- inspecting condoms and condom wrappers for signs of tampering, such as holes or tears;
- switching to a form of birth control that cannot be tampered, such as an IUD, injection, vasectomy, or other forms a medical professional may recommend;
- and other methods an advocate or doctor could recommend.
This information was adapted from Addressing Intimate partner violence Reproductive and Sexual Coercion: A Guide For Obstetric, Gynaecological, Reproductive Health Care Settings The American Gynaecologists (ACOG) and Futures Without Violence.
Pregnancy coercion
Pregnancy coercion includes any behaviors intended to coerce or pressure a partner to become or not become pregnant.Pregnancy coercion involves various tactics, including verbal threats related to impregnation, coerced sex, refusal to use male-controlled contraception (i.e., condoms, withdrawal), interference with or pressure not to use female controlled contraception (i.e., hormonal methods), monitoring menstrual cycles or gynecological visits, pressure for or against female sterilisation, and monitoring of ovulation.
Threatened or completed physical violence may also be perpetrated against a partner to coerce them to become pregnant.
Birth control sabotage
Birth control sabotage involves tampering with contraception or interfering with the use of contraception.
Birth control sabotage includes removing a condom after agreeing to wear one (also called stealthing), damaging a condom, removing contraception (including vaginal rings, intrauterine devices (IUDS), and contraceptive patches), or throwing away oral contraceptive pills.
Other methods of birth control sabotage include preventing a partner from obtaining or refilling contraceptive prescriptions, refusing to wear a condom, stating that a condom is being worn when one is not, not withdrawing after agreeing to do so, exaggerating the risks of hormonal contraceptives, and not telling a partner if a condom broke or fell off.
Gender and sexual power dynamics and coercion associated with sexual power dynamics are both linked to condom nonuse.
Even women with high sexually transmitted infection knowledge are more likely to use condoms inconsistently than women with low STI knowledge when there is a high level of fear for abuse.
Controlling the outcome of a pregnancy
Controlling the outcome of a pregnancy is an attempt to influence a partner to continue or terminate a pregnancy.This can include abortion coercion, or pressuring, threatening, or forcing a partner to have an abortion or not. A Guttmacher Institute policy analysis states that forcing a woman to terminate a pregnancy she wants or to continue a pregnancy she does not want violates the basic human right of reproductive health.
(Wikipedia)